
Healthcare Insights by John August
Empowerment of Workers Leads to Better Healthcare for Patients
In 2011, a group of workers in a dietary department in a large hospital in San Jose, California voluntarily formed a team . Some were experienced Registered Dieticians, and some were cafeteria workers who served food and cleaned up the kitchen. After a few meetings they published their purpose:
Little did they know when they began their team activities that they would accomplish the following:
- Captured $1.144 million additional revenue through increased diagnosis of malnourished patients admitted to hospital
- Improved absenteeism, from 4.11 to 3.72 days per month
- Zero workplace injuries for three years
- Overtime reduction from 2.4% to 1.9%
- Employee engagement score of 94 (average employee engagement scores across the U.S. in health care is between 30-40)
Most memorable about the work of this team was a presentation I attended of the work they had accomplished together . All members of the team participated in the presentation. When it was time for one of the cafeteria workers to present, she stood in front of an auditorium full of administrators and executives, doctors, nurses, and a wide variety of health care professionals. As she began she faltered, speaking in English which was not her first language, which was Spanish. Other members of the team offered to share her presentation on her behalf. But the woman waived them off, and said that she preferred to tell her part of the story herself, full of pride and focus.
I will never forget that experience. All present understood that there was something far more important going on in the dietary unit based team other than stellar performance. What they experienced was the most important outcome of the team formation and collaboration: empowerment of voice.
Why not everyone?
That team is one of 3,500 unit-based teams across one of the nation’s largest health systems, Kaiser Permanente. Nearly 100% of the frontline staff belongs to unions.
Their work is guided by a set of values and strategies adopted by the unions and the management, and sets forth a commitment to form and support the unit based teams with time to do their work and guidance to learn how to identify patient focused improvement projects.
This example is another central proposition in the posts in this column. Here I share examples of how daily work in hospitals and nursing homes can successfully change the general trajectory of health and healthcare in the United States. It is quite clear to me that if every healthcare workplace was organized like the dietary department in San Jose, we could be living in a different world of health-care.
In doing so, we might even introduce some of the much-needed civility and ethics so badly needed in our dangerously polarized society.
Our national non-system of disaggregated delivery is too expensive, unequal with respect to access and health outcomes based on race, ethnicity, and class. Frankly it is wasteful as it is an undeniable truth that our nation spends more than twice as much money on healthcare than any other country in the world, yet our population ranks about 40th in the world when it comes to the health of our population.
We could say the same about many other seemingly intractable challenges to our security and safety as a nation: housing, education, transportation, climate change, debt, retirement savings, and healthcare defined from early childhood care all through aging and death.
It is through voluntary efforts of doctors, nurses, unit secretaries, technicians, housekeepers, certified nursing assistants, and dietary and housekeeping workers, outcomes for patients can exceed the trends which make up the overall poor outcomes that our families, friends, and neighbors suffer through.
Examples previously highlighted in these columns include:
- The Pro-Active Office Encounter Program in Southern California through which Kaiser Permanente improved colon cancer screenings by 27% in a largely diverse population. This program is a collaboration between doctors, unit secretaries, registrars, and other healthcare team members on a daily basis to alert patients of their need for screenings and diagnostic tests to prevent chronic conditions and preventive disease.
- The staff at Coler Nursing and Rehabilitation Center in New York City developed a “bundle” of diagnostics, observation, communication, and therapeutics early in the COVID-19 pandemic, which reduced Infection Fatality Rates (IFR) from 24.4% to zero over a period of three months (before vaccines were available). This achievement occurred among one of the most vulnerable populations in the nation. At Coler, 70% of the residents are poor black men.
- At North Central Bronx Hospital which serves one of the poorest communities in the United States, patient satisfaction improved from a very poor score of 50 to a near perfect score of 99.
The New Idea that binds these and thousands of other workplace-generated and patient-focused improvements in unionized healthcare facilities together is that the traditional subject matter of collective bargaining in the United States can and must evolve beyond “wages, hours, and working conditions” as established in the National Labor Relations Act (NLRA) of 1935. In these cases, the parties to the labor-management dialogue in these institutions voluntarily added the concept of “collective purpose and improvement” so that the workplace itself becomes the locus of empowerment of the voice and experience of the worker to achieve better outcomes for patients.
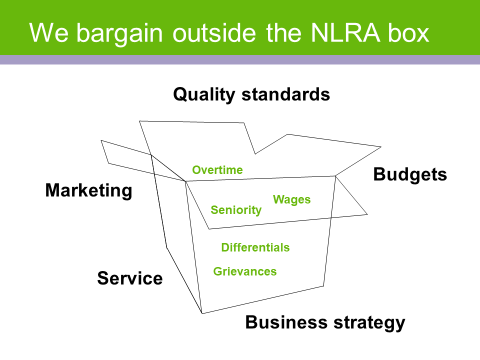
This figure above depicts the nature of bargaining between the Unions and management at Kaiser Permanente.
Doctors Council, SEIU, the largest Union of attending doctors in the country, and NYC Health & Hospitals accomplished something similar. In 2015 and 2020 bargaining, the union and the management agreed and confirmed their commitment to establish Collaboration Councils in all 21 of the public hospitals, nursing homes, and outpatient clinics which serve 1.4 million vulnerable New Yorkers each year in the nation’s largest public health system.
The Collaboration Councils evolved “outside the NLRA box.” The parties made a decision to go beyond the “lawful mandatory subjects of bargaining” and enter the world of non-mandatory issues of bargaining designed by law to preserve management rights and generally to regulate labor relations. The parties agreed that both patient and doctor satisfaction were issues that needed to be addressed. From those discussions, the Councils were established through collective bargaining.
As at Kaiser Permanente, the nature of the collaboration in NYC Health and Hospitals leads people to deep learning about one another and the world they live in. The result is and continues to be the creation of a new culture in the workplace which supports joint learning and focus on initiatives that directly improve patient experience and doctor engagement. Hundreds of patient focused projects to improve patient experience have successfully accomplished breakthrough results, like the ones highlighted at Coler and North Central Bronx Hospital.
It illustrates that the traditional dialogue of overtime, seniority, wages, differentials, and grievances has been voluntarily expanded to include the external stressors and dynamics that impact the traditional bargaining issues. The parties learn that in today’s most challenging world of health care costs, changing demographics, technology, wasteful but inherent competition that stems from our market-driven system of the healthcare industry, that maintaining their ability to provide good wages, hours, and working conditions is deeply challenged. They have learned that to be able to achieve what is traditionally expected, they must act untraditionally!
In so doing, the bargaining opens the parties to new strategic focus and operational change.
And perhaps most interestingly, the collaboration councils and Unit Based Teams (UBT)bring people together in the workplace who would not likely know much about each other outside of work. Doctors, nurses, certified nursing assistants, technologists, unit clerks, the whole health care team engage one another as equals, sharing information, brainstorming, agreeing on problems to solve and using exciting problem-solving tools as equals. Their experience as workers takes on a whole new value and purpose. Their experience flattens a hierarchy of class division.
In 2005 bargaining at Kaiser Permanente, the concept of continuous performance improvement was agreed to in the National Collective Bargaining Agreement. In that section of the Agreement about Performance Improvement, the concept of (UBTs) was introduced.
By 2007, UBT’s were launched in earnest with a guiding patient focused-strategy that all UBTs would follow:
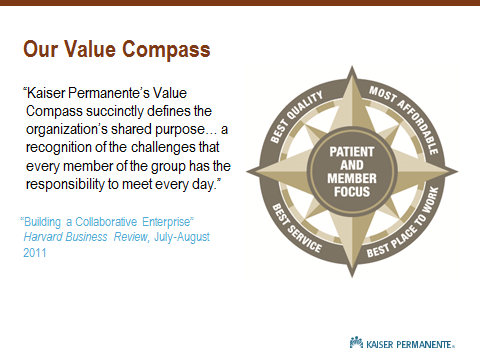
The Value Compass guides the work of every team. So long as their projects fall within one of the points of the Compass, and real progress can be measured, the project is accepted. Through this dialogue, the projects are owned by the workers who perform the work. The results they produce are the result of shared experience. The results are designed to positively impact the patients they serve.
3500 UBTs go to work each day.
It is also the case that improvements in quality and safety, patient experience, finding more efficient ways to do things, eliminate wasteful practices, and capture additional revenue creates a culture of possibility. It also creates real improvement in the very factors that make wages, hours, and working conditions improve: a shared approach to wealth creation and distribution through collaborative work and collective bargaining.
While a minority of healthcare workers in the United States belong to unions, there are nonetheless 2 million healthcare workers who do. At this moment in our history where unionization overall is at its lowest point since the 1920’s, there is a rising interest and activity in unionization. What better time to advance new ideas in the world of work, especially in this time of polarized culture and speech in the face of so many great common concerns from climate change to income and wealth inequality, to the multiple and simultaneous crises in family security, housing, education, debt, and health?
For many years, but especially recently, I have been reading and paying attention to the work of Professor Tim Snyder, the Yale University historian, whose broad area of expertise is Eastern Europe, with special emphasis on Ukraine. In a recent podcast he was putting into context some of the dynamics that have created the current crisis there and what might be done to end it. As part of his analysis, he stated that, “dominant ideas take up the space, but the future depends not on new ideas alone, but ideas that are anchored in values that all can embrace” (Ezra Klein Show, March 15, 2022).
Professor Snyder authored a small book in 2020 called Our Malady (Crown Trade Paperback, a division of Penguin, Random House, New York). The book is a memoir of sorts, about his near-death experience and hospital stay in which he saw first-hand the health care system at its best and worst. In his book, he defines “our malady” in very stark and comprehensive terms: “Our common American malady is a physical illness and the political illness that surrounds it. We are ill in a way that costs us freedom, and unfree in a way that costs us health. Our politics are too much about the curse of pain, and too little about the lessons of liberty” (Our Malady p. 4).
Snyder concludes his thoughts on what to do about American healthcare with this: “We deserve freedom and we need medicine that works. It would begin from people wherever they are, in cities or far from them, near highways or on gravel roads. It would begin from the promise that we have a right to healthcare. Does that sound like a dream? Let it be the American one.” He concludes, “Healing our malady would enrich life, extend liberty, and allow us to pursue happiness, alone and together, in solitude and in solidarity. To be free, we need our health, and for our health we need one another.” (Our Malady page 146).
With Professor Snyder’s moving thoughts in mind, experience has taught me that by challenging ourselves in the workplace with new ideas about values, ethics, and systems, we can “heal our maladies”.
At Kaiser Permanente, labor and management took their efforts at collaboration and improvement beyond self-interest. Theycreated a Case for Change that made it clear that the collective purpose was to create a successful model of healthcare that ought to be adopted across the nation, a health care model that could ensure high quality, affordable healthcare for all.
The Labor Management Partnership made a brief video that was shown across the system to provide an emotional as well as factual reasons for change. You can watch it here.
Kaiser Permanente Changing Work, Changing Lives on Vimeo
While the video was made about 10 years ago, its message resonates today. Little has changed in the nation since that time except we are more polarized and more vulnerable.
In that ten-year period, Kaiser Permanente has been rated as the top health plan in the nation (Consumer Health Ratings, April 13, 2022). The enterprise has grown from taking care of 9 million to 12.5 million people. The unions have grown from 96,000 to 120,000 members. Wages and benefits have increased in what is already the best union contract in healthcare in the nation.
The New Idea was and is to link knowledge and emotion, link people of widely divergent backgrounds in efforts at continuous improvement in which there is equal voice and mutual interest. This has been accomplished on a huge scale.
The New idea was to break away from a long-outmoded idea which separated the way people get by at work and at home, and to embrace and confront the wide world of externality that truly drives how an enterprise functions.
It takes truly New Ideas to end our maladies.
The best place to implement New Ideas is in the world of work, where nearly all of us spend the bulk of our lives.
About the author:
John August is the Scheinman Institute’s Director of Healthcare and Partner Programs. His expertise in healthcare and labor relations spans 40 years. John previously served as the Executive Director of the Coalition of Kaiser Permanente Unions from April 2006 until July 2013. With revenues of 88 billion dollars and over 300,000 employees Kaiser is is one of the largest healthcare plans in the US. While serving as Executive Director of the Coalition, John was the co-chair of the Labor-Management Partnership at Kaiser Permanente, the largest, most complex, and most successful labor-management partnership in U.S. history. He also led the Coalition as chief negotiator in three successful rounds of National Bargaining in 2008, 2010, and 2012 on behalf of 100,000 members of the Coalition.



