
Healthcare Insights: Exclusive Survey Examines Nation’s Largest Public Health System
John August and Lily Mackey Examine NYC Health and Hospitals
Our recent article explored the origin of the NYC Health and Hospitals Collaboration Councils. This column has previously reported on specific successes of the Collaboration Councils in the last 18 months, including outstanding and courageous work during the Pandemic:
The Collaboration Council of the North Central Bronx Hospital | The ILR School (cornell.edu)
Understanding Resilience In The Epicenter Of The Pandemic | The ILR School (cornell.edu)
The Collaboration Councils are facility based forums designed to improve patient experience, doctor engagement, and executive leadership of all of the twenty-two hospitals, major clinics and nursing homes that comprise the nation’s largest public health system, New York City Health and Hospitals.
As of June, 2022, we want to report on the evolution of the Collaboration Councils. We have done this by conducting interviews with both union and management leaders of the Facility Based Collaboration Councils (FBCC) from acute care settings, outpatient settings, and long term care settings. We asked each participant five questions:
- What do you consider the definition of success for your FBCC?
- How have you achieved that success?
- Please share one or two Performance Improvement (PI) projects that you think have been particularly impactful for patients and for doctors?
- If you could envision the future for your FBCC what would that look like with regard to expanded impact and success?
- What suggestions do you have for the System to take full advantage of the achievements of the FBCC’s?
From these interviews, we also asked about improvement projects that they were most proud of and projects that they believe are very impactful for both patients and doctors experiences. We will share examples of outstanding achievements.
And we will illustrate how these experiences align with overall strategic goals of both the Doctors Council and NYC Health and Hospitals (NYC H+H).
We begin with results from the interviews:
- Definitions of success:
a. Encourages doctors and others to get involved in work that they wish to be involved in (Note: a foundational premise of improvement science is to enable frontline staff to participate in improvement projects that reflect problems to solve that they experience directly so long as the projects are generally aligned with overall system strategy).
b. We use a consistently applied form of scientific improvement across the system
c. We see people become passionate about working on ideas that they are interested in
d. Staff are free to create their own path
e. If we clearly create a safe space to openly express the “pebbles in our shoes” without fear of reprisal, we create a psychologically safe environment where real problems get solved
f. Building a culture of safe dialogue is the first metric of success
g. We can “leapfrog” middle management who are often powerless to make change and deal directly with top executives to resolve issues
h. Many problems require a performance improvement approach and there must be collaboration to identify the problems and execute performance improvement projects
i. The FBCC’s can confront structural barriers to encourage more performance improvement
j. Learned many lessons from the pandemic that can be applied going forward
k. We faced “moral distress” in the pandemic which we weathered together
l. Accomplishment of tangible outcomes that are patient centered and of enduring value. The benefits should be long lasting and continue to build upon past success.
m. The increasing collaboration between the front-line physicians and administration. The space is safe to discuss the issues that the physicians face which gets in their way of providing patient care.
n. All participants update one another on challenges and opportunities for improvement: this creates learning and continued interest
o. Many practitioners work on their own or in small settings with little contact with others; the FBCC broadens perspective that would otherwise not occur.
p. We are “building the plane as we are flying it”, so the effort to work on projects together makes that challenge less daunting
2. How have you achieved that success?
a. All meetings start with what the group calls service reports. The opportunity for both sides to provide an update on their respective departments, including the non-physicians at the table. Sometimes the reports are longer than others, but only because the issues or concerns are larger. This is primarily a forum for open communication where both sides can listen to each other. The physicians in this group are not always aware of general information because much of time it is due to how information moves through the organization.
b. It was achieved through meaningful engagement by leadership and direct care providers in all phases of the projects.
c. Having consistent structures, co-chairs of the FBCC, departmental reps all creating projects,
d. Having subcommittees who report out to the entire council; subcommittees include:
i. Quality Improvement
ii. Social committee
iii. Communications/newsletter
iv. Finance
v. “Pebbles in Our Shoes”
e. Choosing projects that have enduring value
f. Our projects helped overcome hopelessness during the pandemic which provides lasting resilience
g. Our collective experience helps us prepare for the next pandemic
3. If you could envision the future for your FBCC what would that look like with regard to expanded impact and success?
a. Encouraged by the impact of collaborative council PI projects in expanding palliative care and improving infection fatality rate, we aligned with a chief medical officer led initiative in our facility to open a post-acute palliative care unit called EQOL unit. EQOL stands for enhanced quality of life and through this unit we aim to bring access of high quality palliative care to our population that is largely affected by social determinants of health. To our knowledge, this model of post-acute palliative care delivery is novel. We have engaged with acute care facilities to provide a pathway of continuity for palliative care, as patients transition from acute to post-acute skilled care. We expect that in the future this work becomes the resource and center of excellence for post-acute palliative care referrals from acute care facilities of H+H.
b. Attendees should participate in either an IHI program, local quality academy, or other forms of how to do a PI Project.
c. Neither Central Office nor Doctors Council should mandate how each Council should work
d. The FBCC should be distinct from the many other quality forums in the system: provide continuous opportunity to hear from frontline providers about ideas that are derived from their own experience that should lead to improvement work
e. Make needed data as easily accessible as possible
f. Find the means to have further communication about the Collaboration Councils internally
g. There is a need for “elbow support”, meaning that more rigorous support for PI projects is essential
4. What suggestions do you have for the System to take full advantage of the achievements of the FBCC’s?
a. Regular senior hospital leadership attendance at the local meetings should be a clear expectation with each hospital held accountable for it to occur. This will further empower the front-line physicians to work on projects and improvements that they see are valuable to caring for the patients. Some lack of participation is noticeable during the system wide meeting sharing, and should be improved for all participating organizations
b. Our health care system has the opportunity to facilitate inter-facility collaboration, by identifying synergy between various projects. Such an integrated approach, can create a patient centered alignment and pathway of care across facilities. For example, a palliative care fellowship program based in hospital which aims to enhance its learning program can collaborate with a post-acute palliative program initiative which seeks to improve patient experience of palliative care. When these projects integrate, they can deliver a continuum of high quality learning and palliative care experience to the patient.
c. Quantify the value of the FBCCs and measure levels improvement and engagement.
d. Integrate around patient centered experience
e. Collaboration with Labor Relations
f. Think along cost effective care, policies, standards
g. Recruitment, retention, as PI projects
h. Improve Performance evaluation processes
i. Improve Credentialing activities
Performance Improvement Achievements of the Collaboration Councils
Since the inception of the Collaboration Councils in February, 2016, there have been continuous and evolving levels of success of Performance Improvement (PI) Projects.
First, what is a PI Project?
It is important to understand that there are at least three, and perhaps more types of PI projects or efforts:
- Quality Assurance. All health care systems must meet regulatory, both external and internal, standards of care. Most healthcare organizations have established Quality Assurance Performance Improvement (QAPI) committees and system wide efforts to comply with these requirements. These are designed as essential efforts to reduce risk to patients of suffering avoidable harm while in the care of a hospital or nursing home, or any federally subsidized health setting (which is just about all)
- Quality Improvement. Most health systems today are adopting various forms of re-engineering of the hospital setting (workplace). LEAN, Six Sigma, and some go so far as to implement the Toyota Production System (TPS) in efforts to encourage continuous improvement. When practiced at their best, the health systems develop systems to engage frontline staff and managers to be the drivers of continuous quality improvement
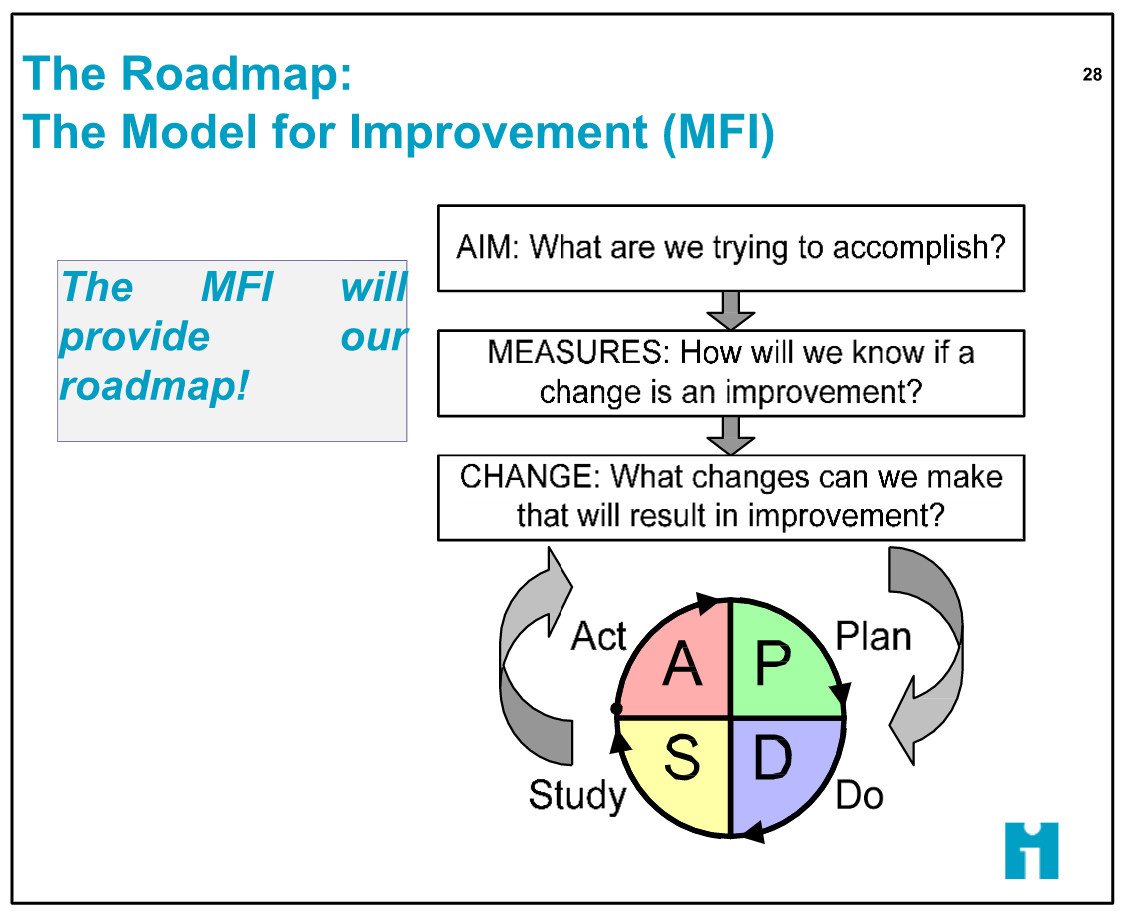
- Whole Systems Change. Advocated most prominently by the Institute for Healthcare Improvement (IHI), quality assurance and quality improvement are integrated into total organizational commitment to the empowerment of frontline teams to select PI projects from their own experience and ensure that these projects are aligned with well understood and widely accepted broad strategic goals. The Whole Systems Approach asks all teams to ask three questions when they identify a project to commit to, and then execute the project with PDSA cycles as illustrated below.
The Collaboration Councils were established through collective bargaining and through the regular joint oversight by leadership of the Doctors Council and senior leadership of NYC H+H. The health system leadership has established Five Strategic Pillars that provide context for PI projects owned and developed by the frontline staff and managers. Doctors Council leaders have supported the Five Pillars as the guide for the development of PI projects. The Five Pillars are:
- Quality and Outcomes
- Care Experience
- Financial Sustainability
- Access to Care
- Culture of Safety
Since 2018, and the alignment achieved on methodology and goals as established through the Model of Improvement, hundreds of PI projects have been developed.
We want to conclude this paper with examples of several of these projects that leaders and frontline doctors told us they were most proud of.
Improving Newborn Screening
AIM: To decrease missed newborn screens at 2-5 days by 50% for all admissions to NICU (neo-natal intensive care unit).
MEASURE: a group of doctors and nurses set out to analyze both people and systems barriers to improvement. They tracked change of new processes over a period of 12 months
CHANGES: they designed a new schedule for ALL babies and designed an in-service for all RNs, addressed workload barriers, addressed lack of awareness of staff of the delay in screening, discussed screening rates during daily rounds
RESULTS: after only four months of plan-do-study-act cycles which addressed the barriers to success, the failure to screen newborns for NICU intervention fell from 79% to 0-1%, which has been maintained, as the new practices were implemented.
Improved Discharge Planning for Mother/Baby Patients
AIM: To improve Patient Satisfaction by engaging patients in timely discharge planning by improving before Noon discharge from 17% to 33%
MEASURE: A group of doctors and nurses brainstormed causes of delays in discharge, and determined that there were a myriad of factors including obtaining birth certificates, clothes, completing safe sleep “talk”, ensuring family had a car seat, resolving any medical issues, scheduling follow up appointments, completing hearing tests. The group also discussed rounding schedules and staffing of both doctors and nurses and made adjustments
CHANGES: Developed a consistently used discharge checklist; developed a consistently developed patient communication checklist; and created an unlimited panel schedule for follow up visits
RESULTS: Over the course of 7 months of PDSA cycles, the group reduced post- Noon discharge from just under 100% of the time to 30% of the time, or a 70% reduction.
Implementation of Social Determinants of Health Screening
AIM: To achieve 80% of patient in-person screening visit, and 70% of in person screen visit who are connected to resources
MEASURES: The group created small group to lead the effort with an advisory group to provide support; held education sessions to discuss importance of screening for social determinants of health;
CHANGES: group developed and administered survey; teams analyzed workflow of patients; and a tracking system was developed
RESULTS: Achieved 95% success of administration of survey and were able to determine top definitions of social determinants to be able to refer for resources:
- Health insurance issues: 71% of respondents
- Food insecurity: 41 % of respondents
- Public assistance: 40% of respondents
- Lack of schooling, English language challenges: 48%
The Collaboration Councils are in their sixth year of implementation and development. Representatives of all the Councils meet quarterly to celebrate successes, learn of strategic priorities, discuss the financial and quality status of the system, and engage in small group discussion where leaders share their experiences with peers. Senior leadership of both Doctors Council and NYC H+H meet regularly to assess progress and advance further resources and time commitments to make the Councils more effective.
While there are always many competing initiatives and challenges that unions and health systems face, the experience of the Collaboration Councils answers some of the questions at least as to how such collaboration and continuous improvement can be accomplished:
- Use the instrument of collective bargaining to think out of the box and address non-traditional subject matter
- Spend resources on process and organizational methods training and education to build consistency of action/implementation
- Include all constituents, and don’t limit continuous improvement efforts to pilots, so as to create system wide acceptance of the need for system wide innovation and improvement
- Align interests
- Create organizational commitment to ensuring a safe place for dialogue, and support the projects and metrics that come from the actual day-to-day experience of frontline staff
None of us know what the trajectory or timing of improved affordability and access to high quality care and improved population health will be in our nation. What we do know is that these issues have festered for a very long time at a policy, regulatory, and legislative level.
We do know that millions of people need care every day, and millions of dedicated people care for them.
The Collaboration Councils are a model that ought to be followed.
About the authors:
John August is the Scheinman Institute’s Director of Healthcare and Partner Programs. His expertise in healthcare and labor relations spans 40 years. John previously served as the Executive Director of the Coalition of Kaiser Permanente Unions from April 2006 until July 2013. With revenues of 88 billion dollars and over 300,000 employees Kaiser is is one of the largest healthcare plans in the US. While serving as Executive Director of the Coalition, John was the co-chair of the Labor-Management Partnership at Kaiser Permanente, the largest, most complex, and most successful labor-management partnership in U.S. history. He also led the Coalition as chief negotiator in three successful rounds of National Bargaining in 2008, 2010, and 2012 on behalf of 100,000 members of the Coalition.
Lily Mackey is an undergraduate in Cornell University’s School of Industrial and Labor Relations. She served as a Research Assistant during the Spring semester, 2022 and assisted on this paper.


